The early history of health Level 7The contents of this whitepaper are published under the Creative Commons Attribution-Share Alike license. Summary
The HL7 protocol dates back to the late 1970s when its precursor was developed at University of California at San Francisco (UCSF) Medical Center
and first implemented in production in 1981.
HL7 v1 and v2 are essentially refinements of the UCSF protocol. X12 and ASTM E1238 have had a large impact on the development of HL7.
The HL7 organization matured from a small ad hoc working group in 1987 into a fullblown standards development organization within its first 5 years.
1. IntroductionThis whitepaper documents some of the history of the creation of the first health Level 7 protocols (small h, capital L) as well as the history of the HL7 organization � from 1979 (precursor activities) up to around 1992, when both the HL7 v2.x standard as well as the organization itself had reached a stable maturity level.Editors note: much of the text is based on snippets of text copied verbatim from papers, websites and various interviews. The history of the ACR-NEMA DICOM standard has been excluded from this whitepaper as it didn't have sufficient impact on the HL7 standard, it probably merits a whitepaper of its own.
2. ContextWhen it comes to the early development of 'Level 7' standards it is of importance to understand the context in terms of software, hardware, and standards being used.Mainframe based medical information systems were initially used in the early 1960s [Ham87]. In the 1970s as clinical support subsystems (minicomputers) evolved for the clinical laboratory, radiology, pharmacy, and for other clinical services, most developed their own separate databases. These created problems for hospitals which used mainframe technology for their financial and registration systems and to a small extent for order entry, results reporting and some other clinical functions. The dominant hospital vendors at that time were SMS and McAuto - all mainframe-based vendors. The clinical support subsystems served the narrower clinical needs of those departments better than the mainframe systems, but they created massive headaches regarding integration. The solution at that time was to connect a terminal from the nursing unit to each of the systems so that a user could use all of the systems by going from terminal device to terminal device. This led to the development of what was called a "front-end" network, which did not involve a OSI Level 7 protocol, but which did allow a single terminal device on a nursing unit to be connected to a network which would allow that device to "log-on" to every computer system attached to the network. These projects used a technology pioneered by the Mitre Corporation called broadband, which at the time referred to coaxial cable similar to that used for cable television, by which multiple communication channels were carried across a single cable. [Netw00, Sim13]. This solved the multiple terminal problem but did nothing for data integration. Such "front end" networks were introduced into some early hospital experiments by Larry Weed at the University of Vermont Hospital in 1976, Octo Barnett in Boston with Bolt Beranek and Newman technology (BBN, creators of much of the technology of the ARPANET, which consisted of just 57 nodes in 1975), and at Walter Reed Army Hospital in 1977. Around 1979 the International Standards Organization (ISO) developed the Open Systems Interconnect (OSI) model and reference base for network systems that specified seven layers for the exchange of data between computers, with each layer corresponding to the same layer in the other computers, although it wasn't until the early 80s that this model was actually being used. In 1976 Ethernet (OSI level 2) was already established over coaxial cables (OSI Level 1) as was TCP/IP (OSI Levels 3 and 4) at the Department of Defense, where work on the ARPANET (precursor to the Internet) started in 1969. Microprocessors (e.g. 8080, Z80) were introduced around 1975. The first microcomputers started to appear, with the IBM PC being launched in 1981, and the Apple II Computer in 1977. Data integration standards were in their infancy at the time: a few high level protocols were used in the context of the ARPANET [Spr78], ANSI X12 (used in finance and logistics) had been created in 1979, ACR/NEMA started their work on DICOM in 1983. A standard for radiology images on magnetic tape was created in 1979. "We struggled with understanding higher level protocols, and typically adapted magnetic tape interchange formats, treating the network as an efficient way of exchanging virtual magnetic tapes" according to Harry Solomon, involved in a non-healthcare LAN project at the time, " This is especially clear in X12, whose flat segment structure is precisely an analog of a mag tape record format." A higher level protocol consists of a data format, as well as a control protocol for such things as query-response handling, acknowledgements and error handling. There were some proprietary batch interfaces between systems, but those were an exception to the rule. Most sites were building their own systems to collect data (e.g. from Lab, Pharmacy, Scheduling systems). [McD90] Interfaces carried a price tag of $100,000 to $500,000 (which would be $360,000 - 1,800,000 in 2013) and could easily take months to create. 3. HL7 PrecursorsThere are two key activities that can be regarded as precursors to HL7. The first set of activities are those by Clem McDonald et.al. leading up to the publication of the ASTM E1238 and E1294 standards, and the other the development and early use of level 7 protocols by health informatics industry representatives like Don Simborg and Tom Pirelli. These activities were closely intertwined, if only because of the fact that the number of interested parties in the field of healthcare informatics was relatively small at the time.3.1 Academia: McDonald et.al.Clem McDonald (Medical Computer Science Research, Indiana University School of Medicine), Ed Hammond (Division of Medical Informatics, Duke University), and other academics first became interested in interface standards through their work with computer stored medical records. The medical record is an assemblage of information from various sources: the clinical lab, the radiology department, the consultant, the nurse, the current physician as well as sources other than the current point of care. Much of that data was electronic even in the mid late 70's but getting it into the computer stored medical record required either manual keying of the data, jerry rigged screen scraping or capture of printer output.Clem McDonald first attempt to stir interest in developing standards for CDI (Clinical Data Interchange) was in the form of an editorial entitled "Grocers, Physicians, and Electronic Data Processing". It stated that the cost of hardware and software was low enough to allow for the use of a computer by most office based physicians, but that the cost of data entry would become prohibitive unless the medical industry developed standards for CDI. The editorial calls attention to the UPC code (the bar code on all grocery products) and applauded the "grocers"' foresight for developing the UPC standard in 1970 � when there was no immediate use for these codes since the computerized checkout counter was a decade into the future. Clem argued that the medical profession should show similar foresight and develop CDI standards. The editorial concludes with "One might argue there are really too few computerized medical record systems to matter so what is the need. We'll let the grocers answer that one." [McD90] The editorial was rejected nine times in the 1981-1983 timeframe. The reviewers argued with Clem on many points, including those that were not actually made: e.g., that "clinical data is nothing like grocery stock", and that "standards would be of no use because physicians did not have computers in their office and never would". The paper was finally published in 1983 [McD83]. Ed Hammond about the general reaction back then related to standards development "That's blue collar work, there is no academic honor in doing it" � there was zero interest. [Ham11] Clem subsequently wrote a paper [McD83a] that provided a starting point for a panel discussion at the Symposium on Computer Applications in Medical Care (SCAMC) meeting of 1983. It contained much of the same arguments as the editorial mentioned above, and stated the following about the actual method for the communication of clinical data (note the absence of LANs): "At the present there are at least two potential media for communicating results between producers and requestors. The first is the telephone. Current modem technology with auto-dialers and auto-answer capabilities could easily support such communication. The second possibility is paper with bar codes. Wand readers and matrix printers that can print bar codes are inexpensive and reliable." At the 1983 SCAMC meeting a group of clinicians, laboratorians and computer scientists started a discussion in AAMSI (one of the forebearers of AMIA) about standards, on how to interest the academic community in standards. Those interested gathered as a task force of AAMSI to formulate a draft standard. Clem McDonald, on the scope of the work: "In order to speed closure, we limited the scope of the initial effort to the interchange of clinical laboratory results. We started with the clinical laboratory on the basis of a variant of Sutton's law - that's where the data is". [McD90] Whilst the group was sympathetic with the desires to encompass many more types of clinical data they believed the chances of success in standards development are improved by starting with a narrow focus. Limiting the focus to clinical laboratory data defines a problem large enough to be important, but small enough to be solved with a few years' worth of effort. They went through three cycles of proposed standards and revisions, and contacted Health Care Financing Administration (HCFA), American Society for Testing and Materials (ASTM), and a number of commercial lab vendors seeking review of the proposed standard. [McD84]
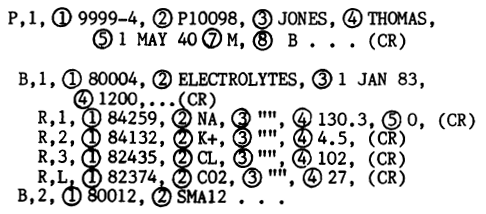
Example Laboratory result. In HL7v2 terms, P became PID, B became OBR, and R turned in to OBX. Note the use of "" for the null value. In the fall of 1984 the task force presented a draft standard [McD84] to an open SCAMC meeting. The panel was moderated by Clem; panel members were Clement McDonald, Gio Wiederhold, Donald W. Simborg, Ed Hammond, Fredrick R. Jelovsek, and Ken Schneider. The participants' responses were a cacophony of disagreement and encouragement. Some argued that even the limited scope of the laboratory was impossibly large, others, that unless the standard covered all medical communications, it was unworthy. [McD90]. For example, Clem McDonald wanted to focus on clinical laboratory interfaces, and Don Simborg held a sincere belief that no single vendor could ever meet the needs of the various clinical departments and clinical specialists, and was primarily interested in creating standards for all of what would be required for an HIS composed of best of breed [Sim88].
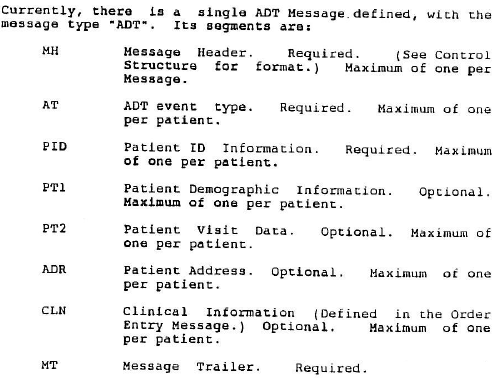
Clem McDonald discusses the history of the development of ASTM 1238 and the HL7 v2 orders/observations messages In 1984 the American Society of Testing and Materials (ASTM) invited the taskforce to organize as a formal subcommittee (known as E31.11 Standards for the Exchange of Clinical Data) within their organization. Ed Hammond: "Clem, Elmer Gabrielli, Octo Barnett, me and others tried to interest AAMSI in standards with no luck. Clem approached ASTM and joined E31, which already existed". [Ham13] "This was an important step because ASTM is one of the few qualified consensus standards forming groups and gave us the tools to develop a formal consensus, with proper procedures and policies" according to Clem McDonald [McD90]. The standard (documented in just 16 pages) was accepted by ASTM and published as E1238-88 (Standard Specification for Transferring Clinical Laboratory Data Messages Between Independent Computer Systems) in 1988. This was the first published balloted consensus standard for clinical data.
Cover page of the ASTM E1238:88 standard. The standard was published in 1988, 1989 was the year for implementation [McD90a]. ASTM E1394, a standard for instrument to lab system interfaces, was subsequently created in close time frame as a simplified version of ASTM E1238. This is still the predominant message standard used between instruments and lab systems. McDonald proposed vocabulary standards for Unite (ISO+) and for some tests and measurements (ASTM) which were incorporated into HL7 Chapter 7. These codes were not sufficient; so later to fill this gap McDonald and colleagues created LOINC. 3.2 Health Informatics Industry: Simborg and TolchinEfforts at the University of California at San Francisco (UCSF) Medical Center�under the direction of Donald W. Simborg (CIO of UCSF), who worked with Steve Tolchin of Johns Hopkins University Applied Physics Laboratory (APL) led to the development of the first true back-end network. The project was initiated in 1976 and put into production in 1981. One of Don's responsibilities at UCSF was to maintain the integrity of the financial and administrative systems and he didn't see the existing solution of multiple terminals on each nursing unit as very practical. This lead to a collaboration between Steve Tolchin at APL and Don Simborg to develop a true "back-end" network at UCSF. Unlike the earlier front-end networks, "back-end" networks did not require a user to be involved in the transaction; instead, the exchange of messages was handled by the computer applications themselves, using a protocol developed specifically for the system [Netw00]. The result was the creation of the first application-level data interchange protocol in health care.The use of "back-end" networks was pioneered by MITRE in the late 1950s for the systems integration of air traffic control systems as part of the SAGE Air Defense system . The SAGE system pioneered a lot of technologies which would gain wider acceptance only decades later [REDM00]. Prior to moving to UCSF Don Simborg worked at Johns Hopkins, and was involved in the development of modular clinical solutions such as radiology and pharmacy. Don started working with computers at APL. APL (associated with Johns Hopkins) had a close relationship with MITRE � which is why Don learned of the possibilities of "back-end" networks through APL.
Don Simborg, the CIO of UCSF as well as the original author of the Level 7 protocol at UCSF. When Don arrived at UCSF in 1976, to be its CIO, the hospital did its billing systems on a mainframe computer owned by the University. Patient identification, ADT, and outpatient registration were paper-based processes. There was a clinical laboratory minicomputer, but paper forms were sent to the laboratory for entry of patient information and clinical laboratory orders and results from the laboratory were printed on paper and sent to the various clinical areas. There were no other computer systems for clinical activities. There was however an increasing interest by various clinical departments to start using minicomputer based systems, leading to an ever greater need for systems integration. It wasn�t long after Don moved to USCF that he started thinking about a �back-end� network. He also found some sources of external funding - a grant from HEW (department of Healthcare, Education and Wellfare) to develop a networked system was the starting point for the implementation phase of such a networked system at UCSF; APL did not get engaged with its development until Don initiated the project at UCSF. "In order to have a network up and running (in test, by 1979, in production by1981, editor) a lot of things had to happen", recalls Don Simborg, when asked about the initial stages of the project (1976-1981). "First, the basic decision to deviate from the 'single-vendor' mainframe-computer-based model had to have been conceived and discussed widely within the administration as this certainly represented a very risky approach. Then, the concept of integration somehow had to be conceived which led to the notion of using a LAN and a level 7 protocol- again a risky approach given the fact that no hospital was using a LAN other than for terminal to host communications (a front-end network, ed.). Then the question of availability of departmental systems was considered (very few existed at the time outside of clinical laboratory). Then the initial departments had to be prioritized which led to ADT/Registration as the key area, followed by Radiology and Outpatient Pharmacy (in addition to clinical laboratory). Then we had to make sure those departments were on board with being the guinea pigs, had budgets available for acquisition, were prepared to devote resources to acquisition and implementation of those department systems. Then we had to actually find the vendors for those systems, help develop the specifications for the applications, acquire the systems and implement them in the departments." "Throughout all of this we had to conceive of the messages that we wanted to have flowing to and from these systems, detail their content, trigger events, error control, etc. (i.e. the Level 7 protocol). Not to mention of course was engaging APL to participate, get their budgets and approvals, get the design, etc. etc. Then we need to fund the project which was a combination of grants and hospital funds. Then we had to negotiate with each of the vendors agreements to implement the protocols. Then we had to test them, modify them as need, re-test them. The working network took testing, re-working, re-testing, and re-design. More importantly, the Level 7 protocol wasn't somehow just delivered to UCSF by APL or anyone else. We had to decide what we needed to accomplish in order to integrate these distributed functions in order for the hospital to function. That took some years of design and specification." In 1981 four minicomputers were connected to the network to exchange transactions between the UCSF registration systems, clinical laboratory, outpatient pharmacy and radiology systems � all built by different manufacturers. The UCSF project consisted of two key parts:
![UCSF systems diagram [Tol81]](../images/ucsf_systems_diagram_Tol81.png)
UCSF Systems Diagram "My team specified the Level 7 protocol which consisted of a broadcast message for ADT/Registration synchronization, and various query-response messages for order entry and results display (text results with the continuation protocol). The specifications included data level definitions � we had extensive discussions with various clinicians, the trigger events and the error controls" according to Don Simborg [Sim13], "We later replaced the ADT/Registration broadcast with a series of point-to-point acknowledged messages. This was the first Level 7 protocol ever used in healthcare to my knowledge. It was only later that I learned about the OSI model and realized that what we were doing was at its level 7. We continued to add computers to the UCSF network and refined the protocol over the years." Mark Shafarman was one of the members of the team that created the level 7 specification. He joined UCSF in 1980, primarily to lead the development of new clinical systems. At the time ADT had already been developed in terms of a level 7 protocol, additional functionality was developed as they went along with the process of systems development.
Mark Shafarman, who started working at UCSF in 1980, comments on the development of the Level 7 protocol. The level 7 protocol was based on "text oriented transmission, of something that looked not too different from what would later evolve into StatLAN and HL7" according to Mark, "Essentially the computer would receive what we now call a text message, process it, and create a type of acknowledgement. The UCSF protocol was a delimited format, the delimiters were different from those ultimately used by HL7 version 2." "The basic transactions look similar to those that can nowadays be found in HL7v2, such as patient registration, acknowledgements, and report. From 1983 onward structured reports were sent to a newly developed patient record system called STOR. Problems, results and labs were the main reports, from those STOR would assemble a patient record. The reports were partially structured, they had a report header that identified the patient, the doctor, the time and the location - all of that was structured. The report itself was structured in sections and paragraphs, and you could actually send a section with coded data."
![UCSF higher level protocol transactions [Ste80]](../images/ucsf_high_level_protocol_transactions_part1_Ste80.png)
![UCSF higher level protocol transactions [Ste80]](../images/ucsf_high_level_protocol_transactions_part2_Ste80.png)
UCSF transactions as defined in 1980, when the scope of the project was still limited to ADT. Note that Queries were called Requests at the time. In the initial year (1981) the network was used to synchronize key patient identification information and registration information among the four systems. Two types of transactions were used: a query/response transaction for demographic and registration information, and a broadcast to the network of demographic and registration information. Network support for these transactions includes error checking, flow control, time-outs, matching of responses to queries, and other functions. [Sim82] Clinical uses of the network began during the second year of the project (1982/1983). [Sim82] UCSF was a 550 bed facility at the time, with 20,000 annual inpatient admissions and 160,000 annual outpatient visits. Utilization of the network was low during the initial year: about 400 broadcasts a day, and about 45 query/response pairs. The transaction rate was expected to increase given the planned addition of several more computers to the network. [Sim82]
![UCSF Request/Response Transactions [Tol81]](../images/ucsf_request_response_transactions_Tol81.png)
UCSF Request/Response Transactions, with expected volume numbers The major problem revealed by the first year's experience relates to the use of the broadcast transaction. The relative importance of this transaction type was not fully appreciated until we had experience with several applications. In view of the high importance of this transaction type, the software design at both the application level (Level 7) and the NIU level (Level 5) were found to be inadequate to 1) insure delivery of the broadcast, 2) to monitor that these broadcasts were successfully delivered to each computer and 3) to provide mechanisms to rebroadcast in case of failure. [Sim82] The broadcast software has been redesigned to use a series of peer-to-peer application level transactions instead of a broadcast of a transaction on the message bus (the NIU level). The original NIUs were replaced (in 1984 or 1985) by Ungermann-Bass Ethernet LAN technology. "In 1984, I approached Ralph Ungermann, the CEO of Ungermann-Bass to see if they would sponsor further research at UCSF", recalls Don Simborg [Sim13], "At the time, Ungermann-Bass was one of the most prominent commercial network companies based in Silicon Valley. Instead of funding research at UCSF, Ralph convinced me to start a company to try to commercialize what we had done at UCSF and helped fund the company. This was the start of Simborg Systems which marketed STATLan, a network-based hospital information system. The STATLan protocol was very similar to the UCSF protocol. Wes Rishel was the VP of Engineering at Simborg Systems and he and I gave seminars in those early years about LANs and the OSI model. We were a struggling start-up company and it became clear that in order to have commercial success there needed to be a non-proprietary standard for the Level 7 protocol. So in 1985, our board agreed to allow the STATLan protocol to be somehow put in the public domain." 4. Early HL7In 1985, the board of Simborg Systems, a struggling start-up company that sold StatLAN, a LAN-based best of breed solution, decided that in order to have commercial success there needed to be a non-proprietary OSI Level 7 healthcare protocol."We weren't trying to be charitable" according to Don Simborg [Sim14], "we were thinking what was in the best interest of the company. So we made the decision to try and organize a standards organization in healthcare." It was felt necessary to create a new organization because the focus of the other standardization efforts at the time was either fragmented, in a different direction or with a different scope than that desired by Don Simborg. He was interested in creating standards for all of what would be required for an HIS composed of best of breed, whereas ASTM E31.11 was focused on lab data and then would expand. [Ham13][Sim87] An 'organizing meeting' was held on March 29/31, 1987 with the aim to create a standards organization. Simborg Systems invited the four hospitals that were the first four StatLAN users: Moses Cone, Auburn Faith Community, Rochester General and Hospital of the University of Pennsylvania (HUP). They also invited the vendors that had agreed to use the StatLAN protocol at those initial four hospitals - mostly vendors of departmental systems. Sam Schultz (CIO at HUP) was asked to be the non-commercial organizer. [Sim13]
Don Simborg, who was the CEO of Simborg Systems, speaking about the creation of the HL7 organization. "I also wanted to invite some industry people who I felt could help promote this, hence the later involvement of people like Clem McDonald, Ed Hammond and Mike Glickman who all were very influential in the process", according to Don Simborg [Sim13], "I was a founding member of the American College of Medical Informatics (ACMI) in 1984 and thus was close to all the major players at that time. Co-founding members included Clem McDonald, Ed Hammond, Morrie Collen, Bruce Blum, Octo Barnett, Fred Jelovsek, Gio Wiederhold - all important people in helping to promote the standard. We were a small community at that time and of course I engaged them in my efforts." Sam Schultz, a very political person, was instrumental in getting the various parties (most of them vendors contracted by HUP) to join the meeting. The initial HL7 meeting, organized by Sam Schultz and Don Simborg had 75 attendees, who represented 20 vendors plus a small number of hospitals and consulting organizations [Sim87]. In order to ensure that meeting would be taken seriously by the press Sam Schultz arranged for about 45 of his colleagues to show up. The actual participants of the meeting numbered about 30, and not 75. At the end of the first day there was a fair amount of despair amongst the meeting organizers (Don, Wes and Sam), about if this thing was going to go anywhere. A lot of people had talked, nothing had coalesced into a set of ideas at that point. Don recalls that it wasn't going well. "People weren't excited about starting an organization, and thought 'who's going to run it, how are we going to fund it', and I remember worrying that the whole thing was going to fall apart. We had about 7 or 8 people that really were pushing this, and some of them were vendors, and others represented hospitals. We actually didn't have the term 'HL7' until the ad-hoc meeting that first night." At the start of the second day Sam announced that a group had split off in the evening and had come up with some ideas. The idea that was presented was that a non-profit organization would be created and that those who were interested would meet within a few months at the Simborg Systems offices. The second meeting, where the first few chapters (2 and 3) were created, was a much smaller meeting, with close to 20 attendees. Most of the content was based on the StatLAN protocol specifications. The third meeting had about 8 attendees. HL7 version 1 was published in October 1987.
John Quinn, who worked at PHS in 1987, comments on the very first and second HL7 meetings in 1987. Neutral Organization"In the early years HL7 looked like a Simborg Systems ploy" according to Don Simborg [Sim14], "it didn't appear to be a neutral body that was available to everybody. We really controlled HL7 in the early years. Wes Rishel and I probably were the main force behind it. We had Sam Schultz, who became the first chair, but he was one of our customers. A lot of the early people were all Simborg Systems related. That wasn't good for HL7." A conscious effort was made to try and pull back, to allow HL7 to go on its own.Don Simborg decided to bow out, and to encourage others to take over some of the leadership positions. He asked Ed Hammond to become the chair of HL7 in 1988; Ed had just taken on some new work, and had to turn him down. Ed did however accept his request in 1989 and became the first non-Simborg Systems related HL7 chair. "Much of the world gives me credit as Father of HL7" according to Ed [Ham13], "I have always been careful to give Don the credit he deserves." MarketingHL7 held a trade-show interoperability demonstration at the August 1988 American Hospital Association (AHA) convention in New Orleans. The testing and validation process prior to the interoperability demonstration was hosted and coordinated by Andersen Consulting, Sue Campbell was the one in charge of the process. They tested the connectivity of each interface as well as its functionality, and then all on an integrated basis before going "live" at a trade show. That work was the first of what has now become known as a connectathon. As such HL7 predated IHE by a couple of years. Subsequently a demonstration involving 7 vendors was held at the HL7 Booth during the HIMSS meeting in February 1989 (in Anaheim, with a total of 1200 attendees). The demonstration was based on version 2.0 and included ADT, pharmacy, laboratory, radiology, and accounting.The following companies were among the participants of these early demonstrations: Sunquest, a pharmacy ancillary vendor based out of Detroit (xxx name?), Compucare (which later became Quadramed) doing ADT, Enterprise OR Scheduling, Cerner Lab, DecRAD, PHS ADT application, and Simborg System's StatLAN product for the nursing unit and to distribute ADT messages. By 1991 permanent demonstrations of HL7 were available at Andersen Consulting's "Hospital of the Future" at the INFOMART in Dallas, and at the Coopers & Lybrand Healthcare Technology Center in Parsippany NJ [Ham91][Ham93]. The aim of these sites was to educate clients on open architecture concepts as well as to provide a marketing tool.

Permament HL7 demonstration at the Coopers & Lybrand Healthcare Technology Center, 1991 The HL7 marketing pitch in the early 90s was primarily related to the cost of interfaces, which was around $100,000 prior to the introduction of HL7, and about $10,000 for HL7 interfaces. Saving money on interfaces appealed to the hospitals, and for the niche player vendors it was their way into the market place. HL7 tried to leverage both. Hospitals were starting to require the vendors to support HL7 - HL7 gained a lot of credibility once it became an ANSI accredited SDO in 1994. Enterprise-oriented system vendorsHL7's marketing pitch was successful to such a degree that the enterprise-oriented system vendors (a.k.a. the "big players") had to take notice. Not only were they loosing quite a bit of systems interfacing revenue, both in terms of licenses as well as maintenance fees, but they also felt the increase in competition of the smaller departmental system vendors.A significant number of enterprise-oriented vendors, motivated by seeing a competitive threat, felt compelled to become a member of HL7 (in the 1989-91 time frame) in order to monitor HL7's activities, to ensure that HL7 stayed away from marketing 'best of breed', and that it focused purely on the development of interoperability standards instead. Early enterprise-oriented vendors to join HL7 included SMS, HBO, Health Data Sciences, Technicon Data Systems (TDS), and Phamis. SMS was the first enterprise-oriented system vendor to join HL7 around 1989. "SMS's primary motive for getting involved was the marketing challenge presented by HL7" according to Mead Walker, who worked at SMS at the time, "and those promoting the best of breed concept. Marketing people at SMS thought it necessary for us to become involved in HL7." "My company, Health Data Sciences, joined HL7 as a counter-balance to claims of 'plug and play' interoperability and 'best of breed' equivalence" according to Gary Dickinson. Their goal was also to debunk the perceived ease and cheapness of setting up interfaces using HL7 as opposed to devising custom solutions � according to these vendors the relative ease of the HL7 solution was being wildly exaggerated. As an indirect consequence of the increasing influence of the enterprise-oriented vendors HL7 dropped its 'puzzle piece' advertisement for "best of breed" showing various system pieces (ADT, scheduling, billing, lab, radiology, pharmacy and other ancillary systems) fitting perfectly together to support an enterprise. HL7 marketing efforts refocused to be solely about the promotion of its interoperability standards. 4.1 HL7 version 1HL7 v.1 was only used for a proof of concept implementation and served to define the content and structure of the standard. The HL7 Working Group has met approximately every 3 or 4 months since the two day initial meeting in March 1987 to develop and review this specification. Three 2 day working group meetings were held in May, June and September to develop the draft standard. They had an attendance of 7-15 people. The version 1.0 draft Standard covered the overall structure of the interfaces, ADT, order entry, and display oriented queries. This draft was presented to a Plenary meeting of the overall group in Tyson's Corner, VA on October 8, 1987. [HL7v1]The aim was to create a standard as soon as possible � this is one of the goals explicitly mentioned in the HL7 v1.0 standard: "A primary interest of the working group is to employ the Standard as soon as possible. To facilitate this, there is no short-term goal to seek accreditation by national or international standards organization. After the Standard has passed through its initial development stage, such accreditation might be most desirable once relative consensus among users and vendors and early operational experience is attained." In October 1987 the highest priorities to standardize were selected being (i) overall transmission control structure (documented in Chapter 2); (ii) admission, discharge, and transfer (Chapter 3); (iii) order entry (Chapter4) (iv) query (Chapter 5); and (v) patient accounts (Chapter 6). [HL7v1] Although the patient accounting system was recognized as very important, the time frame did not allow it to be addressed in the first draft. "A small group, headed by Wes Rishel agreed to write Version 1 of HL7", according to Don Simborg [Sim13], "The group consisted mainly of the original STATLan customers (e.g. Jim Gabler, Bill Lachenauer, et. al.) and original STATLan vendors (e.g. John Quinn, Chris White, et. al.). There were about a dozen total." Members of the working group listed in the HL7 v1 specification are: Sam Schultz (chairman), Ivo Abraham, Lynda Allen, Kenneth Clarke, Jim Gabler, Mike Glickman, Jay Gore, Ed Hammond, David Kingdon, Clem McDonald, Wes Rishel (the main creator of HL7v1), John Quinn (who provided technical leadership jointly with Wes), Don Simborg, B.G. Thompson, and Chris White.
ADT Message Structure as defined in v1. The curly/square braces notation was introduced in HL7v2.0 as a means to define the abstract message structure and was copied from X12. Goals of the Standard [HL7v1], amongst other things "The Standard should be built upon the experience of existing production protocols. It should not, however, favor the proprietary interests of specific companies to the detriment of other users of the Standard". HL7 v1 was effectively based on three sources:
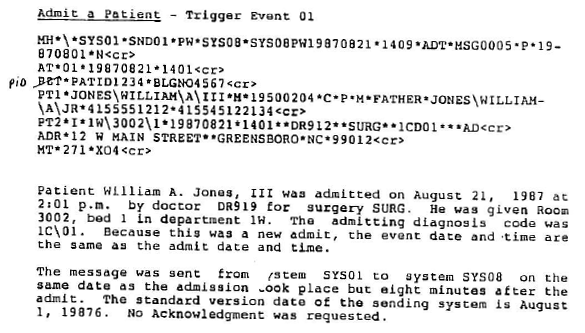
Example ADT message. Note the handwritten correction to "PID" by the reviewer, the segment name had changed during the HL7v1 development process. Enterprise Systems and Simborg were very influential, since they represented protocols that were being used in practice and had been validated by experience. Enterprise provided much of the X12 framework and the experience with batch transmissions. Simborg's influence was related to specific hospital-wide transaction sets and the protocol for on-line exchange. [Hl7v1] The syntax of HL7 v1 was similar to ASTM E31.11, but it was also similar to X12 - and other public and proprietary data syntaxes from three HL7 members (Simborg Systems, Enterprise, Compucare) who offered their intellectual property to the common effort. [Rish99] "After the initial HL7 meeting, I had invited Tom Pirelli [Dry12], the CEO of Enterprise Systems to join the group", recalls Don Simborg [Sim13], "Enterprise was a vendor of hospital departmental systems such as Materials Supply and Surgical Suite and had also developed a proprietary protocol mainly for wide area communications (Enterprise's main focus was communicating between a hospital and various materials suppliers and X12 probably worked for that). Dave Carlson from Enterprise was a member of the Version 1 group. Enterprise also agreed to put its protocol in the public domain and hence, Version 1 was based mainly on the STATLan protocol (which had its start as the UCSF protocol) and some Enterprise protocol." "Tom Pirelli, like the other departmental vendors, had an interest � he was the most important vendor-CEO that helped promote the early HL7. So it was Tom Pirelli and myself who were the 2 vendor companies that worked hard (politically) to get other people involved."

Lab results query and display-oriented response. ANSI X12 is a uniform standard for interindustry electronic interchange of business transactions. The structure of the X12 standard is similar to that of ASTM standards. The HL7 standard is closely modeled on the ANSI X12 Business Data Interchange standard. There are some differences that distinguish the HL7 standard from the ANSI X12 standard [HL7v1]. The ANSI X12 standards apply primarily to batch transmission of data among systems. The HL7 standard differs from ANSI X12 in that it accommodates on-line exchange of individual transactions and LAN interfacing. The standards work of a joint ACR-NEMA working committee (who were working on a precursor of DICOM, known as ACR-NEMA 300, which was published in 1985) was also known to HL7 at the time. The standard didn't have an impact on the functional content of HL7 v1. [HL7v1] 4.2 HL7 version 2Version 2.0 was prepared subsequent to Plenary I in Tyson's Corner and presented at Plenary II in Tucson in September 1988. The direction from the HL7 board was to include billing transactions before pursuing adoption [Rish13]. HL7 v2.0 included billing (HL7 chapter 6). Although targeted to be the first release for actual use in production it served primarily to permit the implementation of a demonstration of the standard and was implemented in only a few settings. Version 2.1 was published in June 1990, and included laboratory results reporting (HL7 Chapter 7) based on the ASTM E1238 specification. [Ham93]Wes Rishel, on using a new major version number: "The decision to skip to a new major version number was informal and based on the concept that it made the standard sound more mature rather than any deep discussion of family characteristics of versions". [Rish13] "The balloting for V2.0 occurred in Washington DC at a Marriott Hotel. We didn't have ANSI rules at the time and Wes conducted the vote" according to John Quinn [Qui13], "It was a "majority hands raised" type vote and not the kind of ANSI balloting with 30 days notice, 30 days to complete a set of written comments and then a negotiation process to arrive at a final count of negatives." After publication of v2.1, HL7 has adopted new formal by-laws and voting procedures. These procedures are modeled on the balloting procedures of other relevant healthcare industry computer messaging standards organizations (e.g., ASTM) and are designed to conform to the requirements of the American National Standards Institute (ANSI). In June 1994, HL7 became an ANSI Accreditid Standards Organization. Mark Shafarman wrote the chapter on master files (Chapter 8) after joining Simborg Systems, which was added in HL7 version 2.2. This chapter was based on the UCSF project: it used an early version of master files. Medix (IEEE P1157 Medical Data Interchange, founded in 1987) was a competitor during the early years. They had a different model for a data interchange protocol - one that was probably more "modern" at the time. They never published a standard, one of the difficulties was agreeing on a data model which HL7 skirted by building one implicitly in the segment structure. Their data modeling effort would ultimately lead to the development of the HL7 RIM [Spr11]. "I consulted with SMS for years and I recall a lunch with the President of SMS where he said they were going with IEEE Medix" according to Clem McDonald, "I argued with him and told him that nothing exists and he should go with HL7. They did." At the time of the development of HL7 v2.0 MEDIX raised a debate about the use of delimiters or name/value pairs. The main concern at the time was that delimited messages were 'too big' for the typical interconnection technology of the day (i.e. 9600 baud serial lines). It came to a vote, with about 12 dissenting vote out of a total of 40. "There was competition between Medix and HL7 for a short time. If we had any hope of getting a standard to be widely used, we needed to have the support of those vendors (e.g. SMS, HBOC, McAuto) which did come slowly and reluctantly" accrding to Don Simborg, "The great debate at the time between Medix (name/value pairs) and HL7 (delimited values) was won by HL7 for two reasons: the mainframe vendors used COBOL which couldn't use name/value pairs and better marketing by HL7." [Sim13] 4.3 ASTM/HL7 harmonizationThe tight relationship between HL7 and the ASTM E1238-88, reporting syntax did not appear until HL7 version 2, and this resulted from a conscious effort by the ASTM and deliberate compromises between the HL7 and the ASTM committees to avoid the evolution of two quite distinct ways to transmit clinical data for the common good. Throughout this collaboration, HL7 transactions always had a much larger scope than ASTM E1238, which dealt only with the ordering and reporting of clinical observations. [Rish99]Somewhere about the timeframe of v2.0 (the fall of 1988) Don Simborg encouraged the merging of the two standards, and orchestrated a meeting between Wes Rishel and Clem McDonald with the purpose of determining if Clem's approach to sending structured lab results was suitable for HL7. [Rish13] Don Simborg commissioned Wes Rishel to organize the "merger", and Wes and Clem spent a day or maybe a day and half holed up in a room at Chicago O'Hare airport, where they worked out the details. [McD13] As a direct result they achieved a common format and the two standards were nearly congruent regarding laboratory results reporting. [McD88] Even though it took a while (at the very latest in 1992, probably earlier than that) to get a formal agreement in place between HL7 and ASTM to duplicate the ASTM content of E1238-88 in HL7 and vice versa, Clem acted as if such an agreement was already in place from the start of the cooperation, and he spent several years conducting parallel meetings in ASTM and HL7 to have the identical content within the different syntaxes of HL7 and ASTM E1238. [Rish13, McD13] Prior to this agreement Orders and Observations were both in Chapter 4; they were split out to 4 and 7 when Clem started the synchronization effort in earnest. "The ASTM committee considered the collaboration a very good thing, because HL7 had such a high participation of members from the health informatics industry compared to the more academic composition ASTM committee" according to Wes Rishel [Rish99], "The sharing went in both directions. Many fields, data types, features and segments were developed first in the HL7 committee and later adopted by ASTM. This sharing was formalized in an official agreement between the officers of HL7 and ASTM, and was helped by the fact that for nearly a decade the ASTM committee and the HL7 orders-results committee had the same chair (Clem McDonald) and an overlapping membership of the volunteers who actually wrote the two standards." "The intent was to keep HL7 and ASTM in sync" accrding to Clem McDonald [McD13], "I chaired both the Observations and orders committee and ASTM 31-11. Think I did manage that for about 2 years. But it was very hard because the balloting was not synchronized, took a ton of time to edit and adjust each version. In the meantime HL7 had gotten traction with industry." "I was chair of the HL7 orders/observation committee from its beginning up to around 1996, and wrote and edited all of the content for many years. I was also chair of the ASTM E31-11 ,the committee that created E1238-88 (and at least 2 other releases) until 1996. Toward the early-mid 90's I think we had 5-6 people at the ASTM meeting and 60 at the corresponding HL7 meeting. I just did not make sense and I did not have the time to keep doing them as parallel and independent things. So I gave up on the ASTM side, because the number of committee attendees was teeny, as was the uptake of the pure ASTM version. Don's plan to do it all, was a hit with industry. I think some ASTM people thought I was disloyal and that the issues of transferring copyrights had been a plot. But it was not; I just ran out of steam." 5. Professionalization of the organisationMike Glickman/Sam Schultz were the primary drivers when it came to the marketing and recruiting effort. Ed Hammond recalls that HL7 handed out balloons to HL7 members - vendors became a member on the spot just to get hold of a balloon.
Mark McDougall about some of the organizational professionalisation aspects. During the first HL7 executive retreat in 1990 (Sept, Chicago), they voted on a set of guiding principles for the organization, most of which still hold true. Ed Hammond took over as the first chair (somewhere around 1990-91). Sam was the first chair and John Quinn was the second. The terms were only one year at that time. About the time that Ed came on board for his first turn at Board Chair is also the time we went to a 2 year chair term. HL7 was managed (in 1991) by an executive committee which consists of a chair, a chair-elect, a past chair, a secretary, a treasurer, an administrator, the technical chair, and a technical secretary. The technical organization is headed by the technical chair and is organized into committees that have responsibility for defined areas of the standard. Each committee is responsible for a chapter of the standard. The committees are control; admission, discharge and transfer; order entry; query; finance: patient accounting; and ancillary data. A quality assurance committee coordinates the overall structure of the standard among the various chapter committees. Other committees are defined for the purposes of supporting the understanding, promotion, and implementation of the standard. These committees include demonstrations, implementation, documentation, and publicity. Another committee exists for the purpose of coordinating the convergence of the activities of HL7 with those of ASTM and IEEE P1157 Medical Data Interchange (MEDIX). [Ham91] In 1991 the organization moved from having an 'executive committee' to a board. The first business plan and budget for HL7 were also written in 1991; the first bylaws were created by Philip Caillouet. The first budget was $105,000. That was the goal, strictly funded by membership revenues. In September of 1991 HL7 signed a administrative/management support contract. "The main objective was to make HL7 viable. There was clearly a need, if they wanted to open an office an operationalize an HL7 organization, but HL7 didn't have any money" according to Mark McDougall, who was hired as the executive director, "Ed Hammond approached Rich Corell ,who was then the president of CHIM, with a request whether he could help HL7 to open up an office. The contract that was pitched was that HL7 would fund one position (Mark McDougal) and a secretary, but HL7 would only ask for half of Marks time. The first thing that I launched was a membership structure with membership dues. They had a short list of about 30 companies and hospitals, that they (the board, ed.) thought would be willing to fund it, and if it didn't fly, HL7 would have folded 12 months later. But it did fly, and as HL7 grew its revenue stream, we were then able to afford additional professional staff." Prior to the creation of an HL7 office the only way to get a copy of the then standard was to fax in a request. The person that would go to the fax machine was a former employee of Sam Schultz named Aarne Elias. He had a fax machine in his dining room and would receive a request for a copy of the standard once or twice a month. He'd read the fax, make a photo copy of the standard, and then he'd mail it out with an invoice for $25, or $50, in the hope that someone would then actually pay the invoice, though they already had the material.
HL7 Board, August 1992. Front row (Left to right): Phil Bartleson, Ed Hammond, Sue Campbell, Dave Carlson, John Quinn. Back row: Philip Caillouet, Wes Rishel, Mike Glickman, David Kates, Mark McDougall. Some of the early HL7 meetings were co-located with MEDIX and ASTM E.31, there were no joint meetings. Many of the people were the same however for MEDIX, ASTM and HL7. By the mid 1990s the number of attendees of WGMs had risen from 5-12 (HL7 v1, 1988), 75 (HL7 v2.1, 1990) to 300 (HL7 v2.2). "For the first few years (early 90s) we had about 100 attendees at WGMs, and about 6 committees that would actively meet" according to Mark McDougall, "Every morning at the general session, a representative from each committee would get up in front of the room, and take about 2-3 minutes to highlights the topics they were going to discuss that half-day. After these presentations I then would ask 'well, so how many people are going to ADT? How many to Control/Query?' Based on which group had the most hands up we would allocate the rooms. We didn't only do this every morning, we also did it after lunch." HL7 used a graphic of a jigsaw puzzle showing the names of the organizational members on the pieces of the puzzle. The underlying theme was that HL7 was the path for interoperability, a glue that held it all together. Hospitals were requiring the vendors to support HL7. That's how HL7 went from an idea to a funded organization. 6. International aspectsIn the late 1980s CEN, the European standards body, had initiated a standardization effort for messages in healthcare based on the EDIFact standard. That, and the fact that HL7 was generally regarded as being very American, and was not an "officially" recognized SDO, hampered adoption in some countries.The initial focus of the UK was on the CEN standards (the HL7 UK affiliate was founded in 1997). "I got excited about interoperability back in 1987, which was the year that EDIFACT became an international standard and both MEDIX and HL7 were founded" according to Tim Benson. "I think I attended my first HL7 meeting in Dallas in early 1988. I organized a meeting in the UK in 1988 which general to interoperability standards. The original UK interest was in IEEE Medix, and then in developing European Standards (CEN TC251)." Bert Kabbes (Coopers & Lybrand Healthcare, the Netherlands) learned of HL7 during a Coopers & Lybrand meeting on November 1st, 1990. George Ahlin (who managed the permanent HL7 demonstration at Coopers & Lybrand Healthcare Technology Center in Parsippany NJ) presented an overview of HL7 v1 during that meeting. Bert recognized that HL7 would help solve some of the interoperability challenges faced by Dutch hospitals. Bert Kabbes subsequently organized a number of 'study tours' (an -almost- annual event from 1991 up to 2002) to enable Dutch organizations to gain knowledge about HL7. These study tours were mostly comprised of a series of on-site visits to US hospitals. The 1991 study tour had 8 representatives of healthcare provider organizations. This study tour involved a HL7 v2.0 training course by Mike Glickman, a visit of the permanent HL7 demonstration at Coopers & Lybrand Healthcare Technology Center, and on site visits to Cabrini Medical Hospital, Fox Chase Cancer Center, Moses Cone Hospital and Duke University Hospital. During this initial study tour an informal 'HL-7 Initiative Committee the Netherlands' was created on the final day of the study tour (Sept.27th 1991). The Dutch HL7 Initiative Committee held a Dutch meeting in January 1992, with 100 attendees, with the aim to inform both the provider as well as the vendor community about the HL7 protocol. Main topic of discussion: why HL7 instead of EDIFACT? Later that same year CEN let it be known that they were against HL7 being introduced in Europe, this was after all a US standard. The first Dutch HL7 v2.1 ADT interface between the Raet HIS and the Philips Labosys laboratory system went live in December of 1992 at the Merwede Hospital in Dordrecht (Jos Baptist). All those involved in the creation of this interface were active members of the Dutch HL7 Initiative Committee which greatly eased the actual implementation effort.
Bert Kabbes, founder of HL7 the Netherlands. A letter was sent to the HL7 executive committee in March 1992 to establish some kind of formal relationship between this Dutch Initiative committee and HL7 itself. This initiated a discussion within HL7 that ultimately led to the creation of the HL7 Affiliate agreement, which was authored by Bert Kabbes, Ed Hammond, Philip Caillouet, Joachim Dudeck and Mark McDougall. The meeting that sparked the beginnings of HL7 Germany took place in 1991 � Joachim Dudeck (Head of the Medical Informatics Institute, G�ttingen) and Bernd Blobel (CIO of Magdeburg University Hospital and Head of the Medical Informatics Department) held a strategy discussion on Hospital Information System architectures. "Joachim Dudeck showed me a copy of a thin document (HL7 version 1) distributed by HP talking about the HL7 endeavor" recalls Bernd Blobel. "He asked me whether I�d already seen this specification. Because the Magdeburg University Hospital was at that time implementing a new Hospital Information System I had received this and some other documents about HL7 as well. Joachim was interested in my opinion and I answered: 'It�s still very immature, the philosophy of the approach however is really interesting'. We decided to engage in this endeavor, aiming to improve and push the HL7 approach." As it happened Joachim Dudeck and a couple of his colleagues visited Ed Hammond at Duke University Hospital one week prior to the visit by Bert Kabbes and the Dutch delegation in September 1991. Bert Kabbes wasn�t aware of any interested parties from Germany, and he made sure to contact Joachim to compare notes. "He was in a university environment, and had a different interest at the time, which was the research side", according to Bert Kabbes, "he didn�t establish a group � that only happened at a later point in time." On March 27-28, 1992, Joachim, with support of Anderson Consulting Germany and Bert Kabbes (Coopers & Lybrand, the Netherlands), organized a HL7 Workshop in G�ttingen, with a sizable representation of the medical informatics community as well as the software vendor community in attendance. As a result of that meeting Joachim launched the Working Group "HL7" within the German Medical Informatics Association GMDS. At its working group meeting on November 30th through December 1st 1992, the creation of a German HL7 User Group ("HL7 Benutzergruppe in Deutschland e.V.") was approved, which was subsequently founded on March 2, 1993. HL7 Germany was formally established about two months prior to HL7 Netherlands, which is why HL7 Germany was the first organization to sign the affiliate agreement, followed by HL7 Netherlands.

HL7 session at Medinfo 1992 in Geneva. Front row, from left to right: Unknown1, Unknown2, Ralf Bucholz, Hans-Dieter Brinkwerth (w/ sweater), Joachim Dudeck (founder of HL7 Germany), W. Ed Hammond, Jack Harrington (IEEE MEDIX), Clem McDonald, Sam Schultz II (initial HL7 chair), Bert Kabbes (founder of HL7 Netherlands), Jaap Noothoven van Goor, Unknown8 (w/ blue dress, Honeywell Bull Netherlands), Unknown9 (w/ brown suit), Tim Benson (far right, w/ pink tie). Others include Cees Molenaar (directly behind Bert Kabbes), Jacob Hofdijk (behind/right of Bert Kabbes), Arie Elsenaar (behind/left of Clem McDonald), Morihide Nagata (behind/left of Hans-Dieter Brinkwerth), Guido de Moor (right/behind of Unknown1), Scott West (the HL7 International Chair, member of MEDIX and TC251 WG 3, behind/left of Joachim Dudeck). The former CEN TC 251 Chair Gunnar Klein successfully intervened at DIN (the German standardization organization) to hinder HL7's accreditation as a formally recognized national standards, but he could not prevent the creation of an Affiliate. HL7 UK began (around 1997) when CEN TC251 lost focus, Georges de Moor resigned as Chair of the CEN TC, and the EU refused to provide any more funding. CEN (and European SDOs such as BSI) were primarily interested in creating as many standards as possible in order to generate revenue. They weren't focused in implementation, training or testing. HL7 was felt to be a better organization to go forward, to create global standards that were fit for purpose. The key movers were Dr Leo Fogarty and Dr David Markwell. 7.SummaryThe development of health Level 7 protocols started during the late 1970s when relatively cheap microprocessors became available leading to a LAN infrastructure and a communications bus. LAN/WAN technology was not new, it had been pioneered by the US Department of Defense in the early 1960s. A communications bus allows for the development of application-to-application (level 7) protocols; such communications are optimized if all systems use one and the same protocol.Don Simborg, about the history of the HL7 v1/v2 standards: "The HL7 protocol dates back to the late 1970s when its precursor was developed at UCSF and first implemented in production in 1979 (editor: testing in 1979, production 1981). The STATLan protocol was a refinement of the UCSF version and V1 of HL7 was just another refinement of that. Although the protocol wasn't called "HL7" until 1985 or 1986, it was essentially the same basic model that was in use since 1979 and was the only Level 7 protocol in actual operation in hospitals with multiple vendors using it at that time." Those interested in the development of healthcare Level 7 differed in opinion as to what the best approach would be to creating such standards: (i) start with standardization in one area, and subsequently branch out to other areas (e.g. Clem McDonald and ASTM E31.11), or (ii) standardize everything at the same time, because partial standardization would hamper adoption (e.g. Don Simborg and HL7). At a later stage, and to the advantage of all parties concerned, the work of ASTM E31.11 was effectively merged with HL7. "In retrospect, it is possible that doing HL7 under ASTM or ANSI or some other existing organization would have been better than going it alone" according to Don Simborg, "but at the time, our focus and struggle was with the healthcare vendors and healthcare providers to try to get them to even understand why this was important." The HL7 organization spent a lot of time during the first few years on reaching out to both the vendor as well as the academic community � many presentations and demonstrations were held at various meetings. By 1990 the number of known implementations, the number of members, and the number of attendees at WGMs had reached such a level that a restructuring of the organization became a necessity, both in terms of process (e.g. ANSI accreditation) as well as in terms of organization (e.g. hiring staff, create formal budgets). Much of the organizational structures and processes have remained the same ever since then. 8 AcknowledgementsThe author would like to thank Don Simborg, Clem McDonald, Ed Hammond, Wes Rishel, John Quinn, Mark Shafarman and Mark McDougall for their willingness to be interviewed at length about their recollections. Tim Benson, Bert Kabbes, Bernd Blobel, Sue Campbell and others provided information about specific parts of this document.8. References
About Ringholm bvRingholm bv is a group of European experts in the field of messaging standards and systems integration in healthcare IT. We provide the industry's most advanced training courses and consulting on healthcare information exchange standards. |


